In US v. Caronia, 703 F. 3d 149 (2d Cir. 2012), a pharmaceutical sales representative, Alfred Caronia, appealed a judgment of the United States District Court for the Eastern District of New York, which convicted him of conspiracy to introduce a misbranded drug into interstate commerce in violation of the Federal Drug and Cosmetic Act (FDCA). Caronia contended that he was convicted for his promotion of the off-label use of an approved prescription drug (Xyrem). According to Caronia, he was convicted for his speech, in violation of this right to free speech under the First Amendment.
The United States Court of Appeals for the Second Circuit, in an opinion authored by Circuit Judge Denny Chin on December 3, 2012, agreed with Caronia and vacated the judgment of conviction. In reaching this decision, the Court reviewed and considered the Supreme Court’s opinion in Sorrell v. IMS Health, Inc., 131 S. Ct. 2653 (2011).
In determining whether there was speech restrictions on pharmaceutical marketing, the Court in Sorrell engaged in a two-step inquiry. First, the Court considered whether the government regulation restricting speech was content- and speaker-based. If it was, the regulation was subject to heightened scrutiny and “presumptively invalid.” The second prong the Court considered was whether the speech was protected by the First Amendment.
In applying this inquiry in Caronia, the Court determined that the FDCA’s misbranding provisions to prohibit off-label marketing is both content-based and speaker-based, and thus, subject to heightened scrutiny. The second prong required applying a four-part test, originally set forth in Central Hudson v. Pub. Serv. Comm’n of N.Y., 447 U.S. 557 (1980). More specifically, in order to warrant First Amendment protection: (1) the speech in question must not be misleading and must concern lawful activity, (2) the asserted government interest must be substantial, (3) the regulation must directly advance the governmental interest asserted, and (4) the regulation must be “narrowly drawn” and may not be more extensive than necessary to serve the interest.
Although the majority found that the government’s construction of the FDCA as prohibiting off-label marketing meets the first two parts of the Central Hudson test, the majority found that it does not withstand scrutiny under the third or fourth part. Thus, the majority held that the government cannot prosecute pharmaceutical manufacturers and their representatives under the FDCA for speech promoting the lawful, off-label use of an FDA-approved drug. Circuit Judge Debra Ann Livingston, finding, among other things, that the third and fourth part of this test was met, filed a vigorous dissent.
Following a hearing last month, the Pennsylvania Senate has passed the Benevolent Gesture Medical Professional Liability Act. Under the Act, statements and acts of contrition by healthcare providers, if made prior to the initiation of medical malpractice litigation, will be inadmissible in subsequent legal proceedings.
Formerly known as Senate Bill 379, the Act had been previously tabled in the Senate through the end of the 2012 legislative session after being passed by the Pennsylvania House of Representatives in 2011. In its original form, the Act prohibited the admission of not only benevolent gestures by healthcare providers, but also admissions of fault or negligence. While sixteen other states have already passed laws deeming such statements to be inadmissible, the bill came under fire in the Senate, as critics argued that it would have prohibited an apology by a physician who had “been on an all-night bender and who revealed that his or her mental state might have contributed to a medical error.” The Act was therefore modified to exclude admissions of fault or negligence, therefore making them potentially admissible in medical malpractice proceedings.
With a new version in place, the bill will now return to the House of Representatives for approval. Hearings are slated to be conducted sometime in the Fall of 2013.
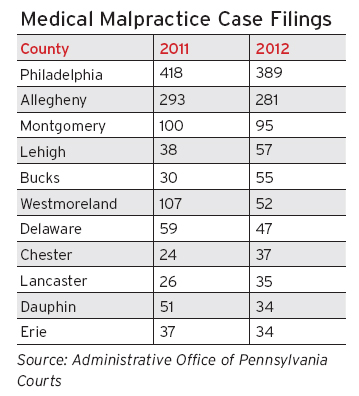
According to statistics recently published by the Administrative Offices of Pennsylvania Courts, 1,508 medical malpractice cases were filed in Pennsylvania in 2012, down 167, or approximately 10%, from the previous year.
This number represents a 44.8% decline from the average number of filings seen from 2000 to 2002, which was right before the Supreme Court’s enactment of several reforms aimed to curtail medical malpractice filings across Pennsylvania. These reforms consisted of requiring such cases to be brought in the venue where the cause of action arose, and a certificate of merit from a medical professional to be obtained prior to filing.
Overall, 133 cases were tried to verdict throughout Pennsylvania, with a total defense verdict rate of almost 80%. Of those cases, 27 were tried in Philadelphia County, with 14 being found in favor of the defense, representing a defense verdict rate of 52%. A 100% defense verdict rate was seen in Montgomery and Chester Counties, which tried 19 and 7 cases, respectively. 6 of 8 cases tried in Delaware county found in favor of the defense, representing a 75% defense verdict rate. Allegheny County saw 10 cases tried to verdict, with 9 finding in favor of the defense.
A comparison of the year-to-year filings in Pennsylvania’s largest counties is as follows:
In an opinion authored on May 17, 2012, by the Honorable Eduardo C. Robreno, Jr., the United States District Court for the Eastern District of Pennsylvania held that under Pennsylvania law, strict liability cannot be imposed on manufacturers of prescription medical devices.
The underlying case of Kee v. Zimmer, Inc., 817 F. Supp. 2d 405, 89 A.L.R. 6th 785 (E.D. Pa. 2012), involved a plaintiff who underwent knee replacement surgery in both knees for treatment of arthritic pain. Integral to the surgeries was a medical implant device manufactured by defendant. Following the surgery, plaintiff experienced persisting knee pain secondary to a loosening of the implant’s component parts. As a result, plaintiff was forced to undergo a revision surgery to correct the implant.
Plaintiff subsequently brought suit against the defendant manufacturer, alleging defective design, failure to warn, negligent design and manufacture, and fraud. Pursuant to diversity jurisdiction, defendant removed the case from Pennsylvania state court to the Eastern District of Pennsylvania. Thereafter, defendant moved for dismissal of all non-negligence claims, including those sounding in strict liability, pursuant to comment k of the Restatement (Second) of Torts § 402A.
On review of defendant’s motion, the Court noted that while Section 402A imposes strict liability on sellers of “unreasonably dangerous products,” an exception is provided for those products which are designated as “unavoidably safe.” Specifically, the Court drew upon the articulation of this exception within Pennsylvania state law, in particular its application to prescription drugs, noting that “where the adequacy of warnings associated with prescription drugs is at issue . . . the manufacturer’s negligence is the only recognized basis of liability.” n v. Richter 3 A.2d 888 (Pa. 1996).
According to the District Court, while the Supreme Court of Pennsylvania had not yet extended the Section 402A exception to prescription medical devices, the Pennsylvania Superior Court, as well as many courts outside Pennsylvania, had already done so. The Court thereby found such precedent sufficient to conclude that “as a matter of Pennsylvania law, there is no strict liability for harm caused by medical devices.” Notably, in recognizing what it termed as a “blanket exception” within Section 402A, the Court refused to allow for a “case-by-case, product-by-product analysis” to determine whether the medical device at issue was unavoidably unsafe. Thus, defendant’s motion was granted and plaintiff’s claims for strict liability were dismissed.
In accordance with the recently launched “National Physician Payment Transparency Program,” also referred to as the “Sunshine Act,” the Centers for Medicare and Medicaid Services (CMS) will begin publishing online searchable information with regard to physician and hospital payments and ownership interests.
Information reported under the Sunshine Act is set to include payments made to physicians by manufacturers engaged in the production of products eligible for payment under Medicare, Medicaid, of the Children’s Health Insurance Program (CHIP). Financial relationships among physicians, their immediate family members, and manufacturers/group purchasing organizations will also be reported, including those in the form of stock, stock options, partnership shares, and memberships in limited liability companies. The Sunshine Act will also require reporting of payments, compensation, expenses, and other contributions given to physicians on behalf of manufacturers/group purchasing organizations, irrespective of whether they are related to a covered drug or device.
In light of the growing concerns over conflicts of interests in patient care and research, the Sunshine Act is intended to increase transparency within the health care field, as well as facilitate increased prosecution under fraud and abuse statues like the Stark Law, anti-kickback statutes, and the False Claims Act. Generally, these laws impose civil and criminal penalties on physicians for a) referring patients to health care services in which the physicians or their immediate family members have a financial interest, b) offering or accepting payment for referrals of Medicare or Medicaid services, or c) presenting a false claim for government payment.
While physicians are not required to take any affirmative action in response to the Sunshine Act, physicians are encouraged to register with CMS so that they may be given the opportunity to review any information before it is published. Specifically, the Act provides a 45 day notice period for the information to be reviewed and, if necessary, corrected. If the 45 day period lapses without a review by the physician, the information may still be reviewed and disputed, albeit at the risk of not having the changes reflected immediately.
Further information on the Sunshine Act can be found by visiting the CMS website, HERE.